Annual Summary of Disease Activity:
Disease Control Newsletter (DCN)
Related Topics
Contact Info
Sexually Transmitted Diseases, 2013
STD Diseases on this page:
Chlamydia
Gonorrhea
Syphilis
Chancroid
Surveillance for gonorrhea and chlamydia are monitored through a passive surveillance system by receiving patient case and laboratory reports. Active surveillance for syphilis involves immediate follow-up with the clinician upon receipt of a positive laboratory report. Cases of chancroid are monitored through a mostly passive surveillance system. Herpes simplex virus and human papillomavirus infections are not reportable.
Although overall incidence rates for STDs in Minnesota are lower than those in many other areas of the United States, certain population subgroups in Minnesota have very high STD rates. Specifically, STDs disproportionately affect adolescents, young adults, and persons of color.
Chlamydia
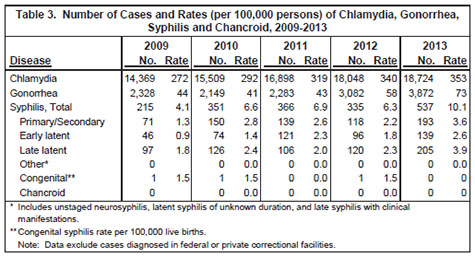
Chlamydia trachomatis infection is the most commonly reported infectious disease in Minnesota. In 2013, 18,724 chlamydia cases (353 per 100,000 population) were reported, representing a 4% increase from 2012 (Table 3).
Adolescents and young adults are at highest risk for acquiring chlamydia infection (Table 4). The chlamydia rate is highest among 20 to 24-year-olds (2,142 per 100,000), with the next highest rate among 15 to 19-year-olds (1,394 per 100,000). The incidence of chlamydia among adults 25 to 29 years of age (843 per 100,000) is considerably lower but has continued to increase in recent years. The chlamydia rate among females (484 per 100,000) is more than twice the rate among males (220 per 100,000), a difference most likely due to more frequent screening among women.
The incidence of chlamydia infection is highest in communities of color (Table 4). The rate among blacks (1,517 per 100,000) is 10 times higher than the rate among whites (158 per 100,000). Although blacks comprise approximately 5% of Minnesota’s population, they account for 23% of reported chlamydia cases. Rates among Asian/Pacific Islanders (289 per 100,000), Hispanics (379 per 100,000), and American Indians (703 per 100,000) are over two to four times higher than the rate among whites.
Chlamydia infections occur throughout the state, with the highest reported rates in Minneapolis (933 per 100,000) and St. Paul (834 per 100,000). While there was an overall increase of 4% across the state in 2013, the greatest increase for chlamydia was seen in the Greater Minnesota area with an increase of 7%. For the first time ever, Minnesota had at least 3 chlamydia cases in every county in the state in 2013.
Gonorrhea
Gonorrhea, caused by Neisseria gonorrhoeae, is the second most commonly reported STD in Minnesota. In 2013, 3,872 cases (73 per 100,000 population) were reported, representing a 26% increase from 2012. This is the highest reported rate of gonorrhea in the last decade (Table 3).
Adolescents and young adults are at greatest risk for gonorrhea (Table 4), with incidence rates of 267 per 100,000 among 15 to 19-year-olds, 360 per 100,000 among 20 to 24-year olds, and 177 per 100,000 among 25 to 29-yearolds. Gonorrhea rates for males (70 per 100,000) and females (76 per 100,000) are comparable. Communities of color are disproportionately affected by gonorrhea, with nearly one half of cases reported among blacks. The incidence of gonorrhea among blacks (611 per 100,000) is 26.5 times higher than the rate among whites (23 per 100,000). Rates among Asian/Pacific Islanders (32 per 100,000), Hispanics (53 per 100,000), and American Indians (165 per 100,000) are up to seven times higher than among whites.
Gonorrhea rates are highest in the cities of Minneapolis and St. Paul (Table 4). The incidence in Minneapolis (359 per 100,000) is over 1.5 times higher than the rate in St. Paul (230 per 100,000), seven times higher than the rate in the suburban metropolitan area (49 per 100,000), and 15 times higher than the rate in Greater Minnesota (23 per 100,000). Geographically in 2013, Minneapolis had the largest increase in cases at 28% and Greater Minnesota had a 27% increase in cases.
The emergence of quinolone-resistant N. gonorrhoeae (QRNG) in recent years has become a particular concern. Due to the high prevalence of QRNG in Minnesota as well as nationwide, quinolones are no longer recommended for the treatment of gonococcal infections. Additionally, the CDC changed the treatment guidelines for gonococcal infections in August 2012. CDC no longer recommends cefixime at any dose as a first-line regimen for treatment of gonococcal infections. If cefixime is used as an alternative agent, then the patient should return in 1 week for a test-of-cure at the site of infection.
Syphilis
Surveillance data for primary and secondary syphilis are used to monitor morbidity trends because they represent recently acquired infections. Data for early syphilis (which includes primary, secondary, and early latent stages of disease) are used in outbreak investigations because they represent infections acquired within the past 12 months and signify opportunities for disease prevention.
Primary and Secondary Syphilis
The incidence of primary/secondary syphilis in Minnesota is lower than that of chlamydia or gonorrhea (Table 3), but has remained elevated since an outbreak began in 2002 among men who have sex with men (MSM). In 2013, there were 193 cases of primary/ secondary syphilis in Minnesota (3.6 cases per 100,000 persons). This represents an increase of 64% compared to the 118 cases (2.2 per 100,000 population) reported in 2012.
Early Syphilis
In 2013, the number of early syphilis cases increased by 55%, with 332 cases occurring compared to 214 cases in 2012. The incidence remains highly concentrated among MSM. Of the early syphilis cases in 2013, 298 (90%) occurred among men; 261 (88%) of these men reported having sex with other men; 46% of the MSM diagnosed with early syphilis were co-infected with HIV.
Congenital Syphilis
There were no cases of congenital syphilis reported in Minnesota in 2013.
Chancroid
Chancroid continues to be very rare in Minnesota. No cases were reported in 2013. The last case was reported in 1999.
- For up to date information see>> Sexually Transmitted Diseases (STDs)
- Full issue>> Annual Summary of Communicable Diseases Reported to the Minnesota Department of Health, 2013