Annual Summary of Disease Activity:
Disease Control Newsletter (DCN)
Related Topics
Contact Info
Streptococcus pneumoniae Invasive Disease, 2015
Statewide active surveillance for invasive Streptococcus pneumoniae (pneumococcal) disease began in 2002, expanded from the metropolitan area, where active surveillance was ongoing since 1995. In 2015, 534 (9.8 per 100,000) cases of invasive pneumococcal disease were reported. By age group, annual incidence rates per 100,000 were 10.3 cases among children aged 0-4 years, 2.5 cases among children and adults aged 5-39 years, 11.0 cases among adults 40-64 years, and 30.3 cases among adults aged 65 years and older.
In 2015, pneumonia occurred most frequently (50% of infections), followed by bacteremia without another focus of infection (29%), septic shock (8%), and meningitis (6%). Fifty-six (10%) cases died. Health histories were available for 51 of these 56 cases; of these, 48 had an underlying health condition reported. The conditions most frequently reported were emphysema/chronic obstructive pulmonary disease (16), diabetes (13), heart failure/congestive heart failure (12), alcohol abuse (9), current smoker (7), solid organ malignancy (7) dementia (7), and atherosclerotic cardiovascular disease (4).
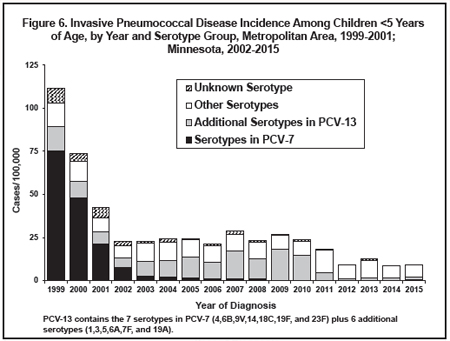
In 1999, the year before the pediatric pneumococcal conjugate vaccine (Prevnar [PCV-7]) was licensed, the rate of invasive disease among children <5 years of age in the metropolitan area was 111.7 cases/100,000. Over 2000 to 2002 there was a major downward trend in incidence in this age group (Figure 6). Rates in each of the subsequent 8 years were level or somewhat higher, although there has not been a continuing upward trend since 2012 (Figure 6). Based on the distribution of serotypes among isolates from these cases, this increase was limited to disease caused by nonvaccine serotypes (i.e. serotypes other than the 7 included in PCV-7) (Figure 6).
In March 2010, the U.S. Food and Drug Administration approved a new 13-valent pediatric pneumococcal conjugate vaccine (PCV-13 [Prevnar 13]) which replaced PCV-7. The new vaccine provides protection against the same serotypes in PCV-7, plus 6 additional serotypes (serotypes 1, 3, 5, 6A, 7F, and 19A). From 2007 to 2010, the majority of invasive pneumococcal disease cases among children <5 years of age have been caused by the 6 new serotypes included in PCV-13 (Figure 6). Since 2011, the majority of invasive pneumococcal disease cases among children <5 years of age have been caused by serotypes not included in PCV-13 (Figure 6).
In 2015, 17% of cases occurring among Minnesotans of all ages, with isolates available for testing, were caused by 3 of the new PCV-13- included serotypes: 3 (11%), 19A (3%), and 7F (3%). In August 2014, the Advisory Committee on Immunization Practices recommended that all adults ≥65 years of age receive 1 dose of PCV-13 followed by 1 dose of 23-valent pneumococcal polysaccharide vaccine (PPSV-23) 6 to 12 months later. Among adults 65 years and older 15% of cases were caused by PCV-13 serotypes in 2015.
Of the 499 isolates submitted for 2015 cases, 98 (20%) isolates were resistant to penicillin using meningitis breakpoints. Using non-meningitis breakpoints, 5 (1%) isolates were resistant to penicillin and 8 (2%) exhibited intermediate level resistance (Note: CLSI penicillin breakpoints changed in 2008; refer to the MDH Antibiogram on pp. 28-29). Multi-drug resistance (i.e., high-level resistance to two or more antibiotic classes) was exhibited in 82 (16%) isolates.
Surveillance for non-invasive S. pneumoniae disease become established January 1, 2016. Cases are detectable through positive urine antigen screening from select sentinel hospital laboratories. Surveillance is limited to Minnesotans aged ≥18 years who reside within the metropolitan area. Retrospective cases through January 1, 2013 were also made reportable. In 2015, 90 non-invasive pneumococcal disease cases were reported. Fifty-five cases (61%) were female. Cases had a median age of 69.5 years, with 25% aged 57 years or younger and 25% aged 81 years or older. Five percent of cases were aged 35 years or younger, with the youngest case aged 24 years. All 90 cases had underlying conditions, with 36 (14%) reporting emphysema/ chronic obstructive pulmonary disease. Other common underlying conditions included 29 (11%) with current smoking, 21 (8%) with history of solid organ malignancy, 18 (7%) with asthma, 15 (6%) with obesity, and 12 (5%) with chronic kidney disease. Two cases died during hospitalization, and 33 cases (37%) required admission to intensive care.
- For up to date information see>> Streptococcus pneumoniae (Pneumococcal Disease)
- Full issue>> Annual Summary of Communicable Diseases Reported to the Minnesota Department of Health, 2015