Annual Summary of Disease Activity:
Disease Control Newsletter (DCN)
Related Topics
Contact Info
Lyme Disease, 2017
Lyme disease is caused by Borrelia burgdorferi, a spirochete transmitted to humans by bites from Ixodes scapularis, the blacklegged tick.
Recently, a new species of bacteria, B. mayonii, has also been identified as a cause of human disease, and 8 cases have been reported in Minnesota residents since 2013. In Minnesota, the same tick vector also transmits the agents of babesiosis, human anaplasmosis, one form of human ehrlichiosis, and a strain of Powassan virus.
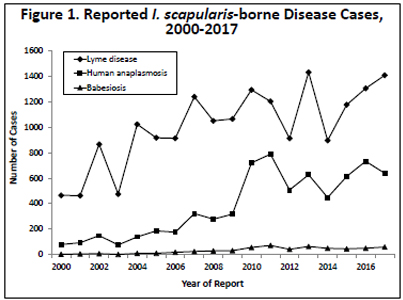
In 2017, 1,408 confirmed Lyme disease cases (25.5 cases per 100,000 population) were reported. In addition, 910 probable cases (physician-diagnosed cases that did not meet clinical evidence criteria for a confirmed case but that had laboratory evidence of infection) were reported. Despite some yearly fluctuations, the number of reported cases of Lyme disease has been increasing, as evidenced by the median number of cases from 2009 through 2016 (median, 1,203; range,
896 to 1,431) compared to the median from 2000 to 2008 (median, 913; range, 463 to 1,239) (Figure 1).
Eight hundred sixty-five (61%) confirmed cases were male, and the median case age was 43 years (range, 1 to 91). Physician-diagnosed erythema migrans (EM) was present in 1,042 (74%) cases. Four hundred sixteen (30%) cases had one or more late manifestations of Lyme disease (including 291 with a history of objective joint swelling, 101 with cranial neuritis including Bell’s Palsy, 11 with lymphocytic meningitis, 10 with acute onset of 2nd or 3rd degree atrioventricular conduction defects, and 7 with radiculoneuropathy) and confirmation by Western immunoblot (positive IgM ≤30 days post-onset or positive IgG). Of the 1,300 cases with known onset dates, onset of symptoms peaked from June through August, with 70% of EM cases experiencing symptom onset in June or July. This timing corresponds with peak activity of nymphal I. scapularis ticks in mid-May through mid-July. The majority of cases either resided in or traveled to endemic counties in north-central, east-central, or southeast Minnesota, or Wisconsin.
- For up to date information see: Lyme disease
- Full issue>> Annual Summary of Communicable Diseases Reported to the Minnesota Department of Health, 2017