Children and Youth with Special Health Needs (CYSHN)
Programs
Contact Info
Neonatal Abstinence Syndrome
People who use substances, most often opioids, during their pregnancy are at risk for giving birth to a baby that experiences neonatal abstinence syndrome (NAS). If a pregnant person uses substances, the drugs can pass through the placenta to the baby. When the baby is born, they no longer receive these substances and can experience withdrawal symptoms. Babies are not born addicted to substances, rather they have a physiological dependence due to substance exposure in the womb.
About NAS
While usually the result of opioid use, NAS can be caused by other substances including stimulants, amphetamines, barbiturates, benzodiazepines and more.
- Both prescribed substances, like oxycodone or methadone, or illicit substances, like heroin can cause NAS.
- The term NAS more broadly captures newborn withdrawal resulting from a wide variety of substances if used during pregnancy, while neonatal opioid withdrawal syndrome (NOWS) focuses specifically on withdrawal from opioid exposure. This distinction helps address the rising prevalence of neonatal withdrawal due to the opioid epidemic.
- Symptoms of withdrawal usually appear within three days of birth but may begin as late as 5-10 days.
- Fever, seizures, tremors (body shakes), high pitched cry, difficulty eating and sleeping, irritability, and other symptoms are common for newborns with NAS or NOWS. They may require a longer hospitalization to manage symptoms.
- While initial symptoms of withdrawal usually resolve within the first 6 months of life, infants may be at an increased risk for long-term impacts, such as developmental delays (not meeting milestones on time).
- Concerns may appear in one or more areas of development: vision, talking, moving, learning, growing, and behaving.
More information about NAS in Minnesota is available on our neonatal abstinence syndrome monitoring system fact sheet.
If you think that you are pregnant or might become pregnant and are currently using substances, it is important to talk to your doctor. Your doctor and other health care providers can give you information on how to safely reduce or stop substance use, provide referrals to substance use treatment, and support you in having a healthy pregnancy. Pregnant people with untreated substance use disorder can discuss their use with their health care provider, and the health care provider is not required to automatically report that use to child protective services, so long as the pregnant person continues to receive regular prenatal and postpartum care after disclosing substance use. Please see Minnesota Statute 260E. 31 Subdivision 1 for additional information and care requirements.
What can I do?
- Talk to your doctor to determine what treatment options are right for you.
- Determine if you may benefit from medication for opioid use disorder (MOUD).
- Consider attending peer-to-peer support groups, 12-step programs like Narcotics Anonymous (NA), counseling, and other community-based programs.
- Attend follow-up appointments to track your baby’s growth and development.
- Enroll in early childhood programs like Family Home Visiting (FHV), Help Me Grow, and the Follow Along Program.
- Learn how substance use may impact your baby while pregnant or breastfeeding on the Mother to Baby website.
Infants diagnosed with NAS are at risk for developmental deficits that can appear later in infancy or childhood. This can include developmental delays, learning difficulty, behavioral concerns, and problems with vision, speech, and language.
It is difficult to separate the role of prenatal substance exposure and environment in the development of long-term health outcomes. For example, infants impacted by NAS often live in high-risk social environments, which can include parental substance use disorder, mental illness, domestic violence, and limited access to health care, food, and shelter. These adverse childhood experiences (ACEs) can negatively impact a child’s health and development. Health outcomes improve when parents receive and maintain treatment for substance use disorder, live in a stable home with adequate access to resources, and have parenting support.
Recommendations
Public health programs are available to support the needs of infants and families impacted by NAS or substance use. Connections to such resources should be included as part of the Plan of Safe Care (POSC). It is important to ensure that the POSC is developed as soon as substance use in pregnancy is identified, or at a minimum, before hospital discharge.
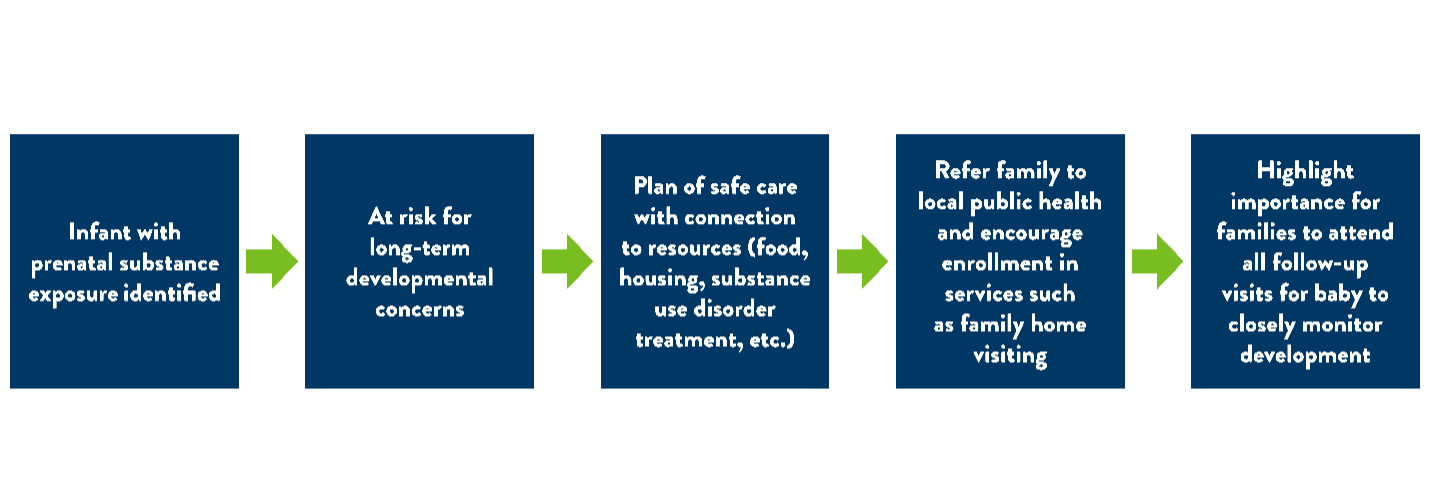
Figure 1: Connection to resources for infant and family.
The rate of babies born in the United States with NAS has rapidly increased over the years. In 2014, it was reported that a baby with NAS was born every 15 minutes.
NAS data in Minnesota is currently collected using hospital discharge data. From 2016 to 2024, there were 3,601 NAS-related hospital visits in Minnesota . This corresponds to a statewide rate of 6.4 per 1,000 live births. The median rate (i.e., the rate in the middle of the overall range of rates) among counties in Minnesota was 3.9 per 1,000 live births. Information on NAS by region of the state and by sex of infant is available in the Neonatal Abstinence Syndrome (NAS) Data brief: statewide and county trends, 2016-2024.
Environmental scan
An NAS environmental scan was conducted by The Improve Group in 2025 in partnership with MDH to better understand the current landscape of NAS in Minnesota. The goal of this scan is to inform ongoing conversations, identify gaps and opportunities, and provide valuable insight to further guide MDH in supporting families, providers, and communities most impacted by NAS.
The findings shared (PDF) reflect a combination of research, data analysis, and firsthand insights gathered through focus groups and interviews. These perspectives offer valuable context, but do not necessarily reflect the official views or policy positions of MDH.
Drug overdose dashboard
The drug overdose data dashboard has information on opioid overdose death, nonfatal overdose, use, misuse, substance use disorder, prescribing practices, supply, diversion, harm reduction, co-occurring conditions, and social determinants of health.
The Minnesota Perinatal Quality Collaborative (MNPQC), a partnership between the Minnesota Department of Health and the Minnesota Perinatal Organization, leads initiatives focused on improving maternal and infant health. The MNPQC led a Mother/ Infant Opioid Substance Use Treatment and Recovery Effort (MOSTaRE), which is now in the maintenance phase. The goal of this effort is to improve identification of pregnant and parenting individuals with opioid use disorder, and to improve support, clinical care, and coordinated treatment through a family-centered approach that maintains the mother-infant dyad. This is achieved through a collaborative effort with providers, hospitals, and stakeholders.
The MNPQC is starting a Community of Learning (COL) project with a focus on the Eat, Sleep, Console (ESC) model of care for infants impacted by prenatal substance exposure. This evidence-based model guides care in managing Neonatal Opioid Withdrawal Syndrome (NOWS). This model empowers the parent as the primary caregiver and uses a holistic approach that minimizes the need for pharmacological therapy, thereby leading to a reduced length of stay in the hospital. This project will take place August 2024- March 2025.
- Early childhood programs to support growth and development
- Resources to help with food, housing, medical insurance and more
- Find a treatment center
- Fast Tracker is a tool developed by the Minnesota Department of Human Services
- FindTreatment.gov
- Substance use disorder: Information, resources, and programs
- Fact sheets
- Can Babies Become Dependent on Drugs? (n.d.). Cleveland Clinic. https://health.clevelandclinic.org/neonatal-drug-withdrawal
- Centers for Disease Control and Prevention. (2021). About opioid use during pregnancy. About Opioid Use During Pregnancy | Opioid Use During Pregnancy | CDC
- Giesel, S., Corey, L., & Wright, N. (2023). Neonatal Abstinence Syndrome: Statewide and County Trends, Data Brief. Minnesota Department of Health. Retrieved from Neonatal Abstinence Syndrome (NAS) Data brief: statewide and county trends, 2016-2022
- Jilani SM, Frey MT, Pepin D, et al. Evaluation of State-Mandated Reporting of Neonatal Abstinence Syndrome- Six States, 2013-2017. MMWR Morb Mortal Wkly Rep 2019;68-10. DOI: http://dx.doi.org/10.15585/mmwr.mm6801a2. Evaluation of State-Mandated Reporting of Neonatal Abstinence Syndrome — Six States, 2013–2017 | MMWR (cdc.gov)
- Kozhimannil, K.B., Chantarat, T., Ecklund, A.M., Henning-Smith, C., & Jones, C. (2018). Maternal opioid use disorder and neonatal abstinence syndrome among rural US residents, 2007-2014. The Journal of Rural Health 35,(1), 122-132.
- March of Dimes. (n.d.). Neonatal Abstinence Syndrome (NAS). Retrieved June 21, 2024, from https://www.marchofdimes.org/find-support/topics/planning-baby/neonatal-abstinence-syndrome-nas
- Merhar SL, McAllister JM, Wedig-Stevie KE, Klein AC, Meinzen-Derr J, Poindexter BB. Retrospective review of neurodevelopmental outcomes in infants treated for neonatal abstinence syndrome. J Perinatol. 2018 May;38(5):587-592. doi: 10.1038/s41372-018-0088-9.