Alcohol and Other Drugs
Alcohol Basics
Alcohol Data
Related Topics
Alcohol and Other Drugs
Quick Facts
Suicide, Alcohol and Opioid Deaths in Minnesota
In 2017, hundreds of Minnesotans died by suicide, alcohol and/or opioids.
- 783 deaths were from suicide
- 636 deaths were from alcohol
- 422 deaths were from opioids
Put into perspective, many small towns in Minnesota have fewer than 800 residents. This is the equivalent of losing an entire town's population each year due to these preventable deaths.
Suicide
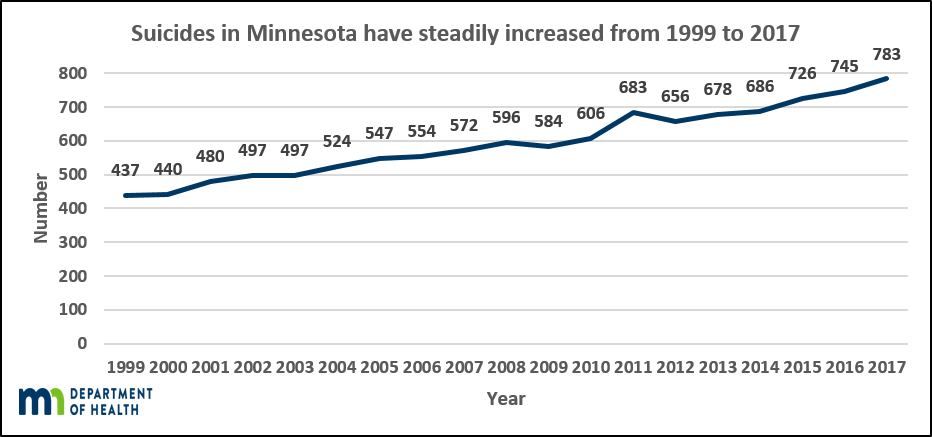
Suicide is the eighth leading cause of death in Minnesota and tenth nationally. From 1999-2017, suicide deaths steadily increased from 437 in 1999 to 783 in 2017. This is an increase of 79 percent. Suicides are not experienced equally across age groups, genders or geography in Minnesota:
- Firearms are the leading mechanism of suicide deaths for males, and account for 54 percent of male suicide deaths.
- From 2016 to 2017, the male suicide rate increased 18 percent from in the Seven-county Metro, but remained lower than the Greater Minnesota male suicide rate.
- Comparing suicide rates by race during the 2013-2017 period, the American Indian population experienced the greatest rate in Minnesota and had a rate nearly two times greater than the national rate.
Suicide is rarely random or inevitable. There is not one single path that leads to suicide. Suicide death is complicated and is often the result of a combination of factors experienced across a lifetime like childhood trauma, serious mental illness, substance abuse, painful loss, exposure to violence, social isolation and loneliness, and easy access to lethal means.
Suicide is preventable. We can decrease the risk of suicidal thoughts and behaviors by increasing access to quality behavioral healthcare, building meaningful relationships, practicing safe suicide reporting and messaging, developing coping skills, and creating safe and supportive communities.
Alcohol
Alcohol is used more often and by more people than any other drug, and alcohol contributes to more deaths, injuries, and illnesses than any other drug. It is also the primary substance used among adults in Minnesota who are admitted to substance use disorder treatment services.
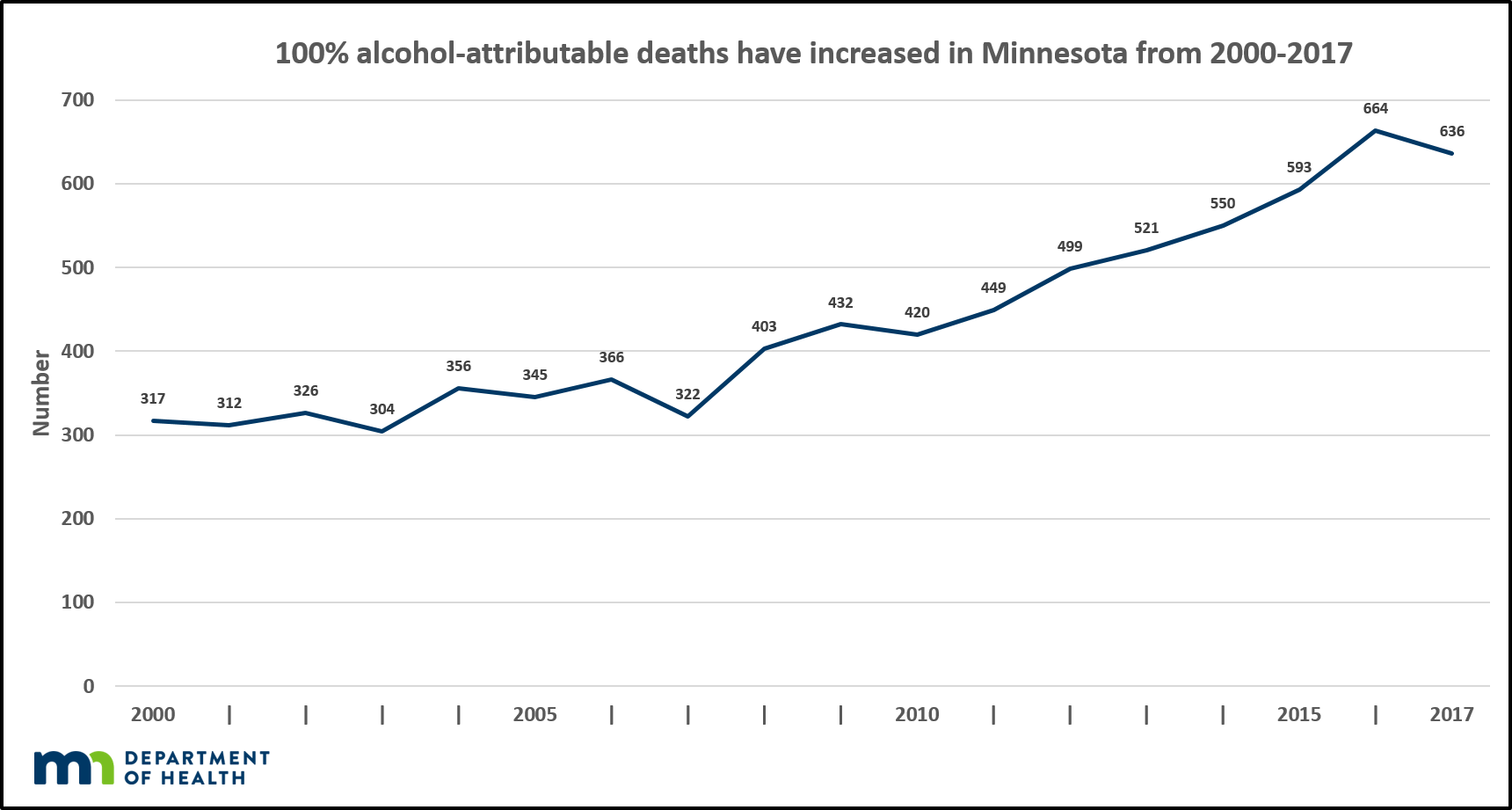
The estimated number of 100% alcohol-attributable deaths has increased over the past 17 years.
- 100% alcohol-attributable deaths increased by 94% between 2000 and 2017.
- The rate of alcohol-attributable deaths increases with age, with the largest increase over time seen among those 50 years and older.
- Men are more likely to die from 100% alcohol-attributable conditions than women.
- In 2012-2016, American Indians in Minnesota died of 100% alcohol-attributable causes of death at rates four times higher than whites (44.1 vs. 10.9 per 100,000). These rates are up from 30.8 and 6.8 per 100,000 for American Indians and whites, respectively, in 2001-2005.
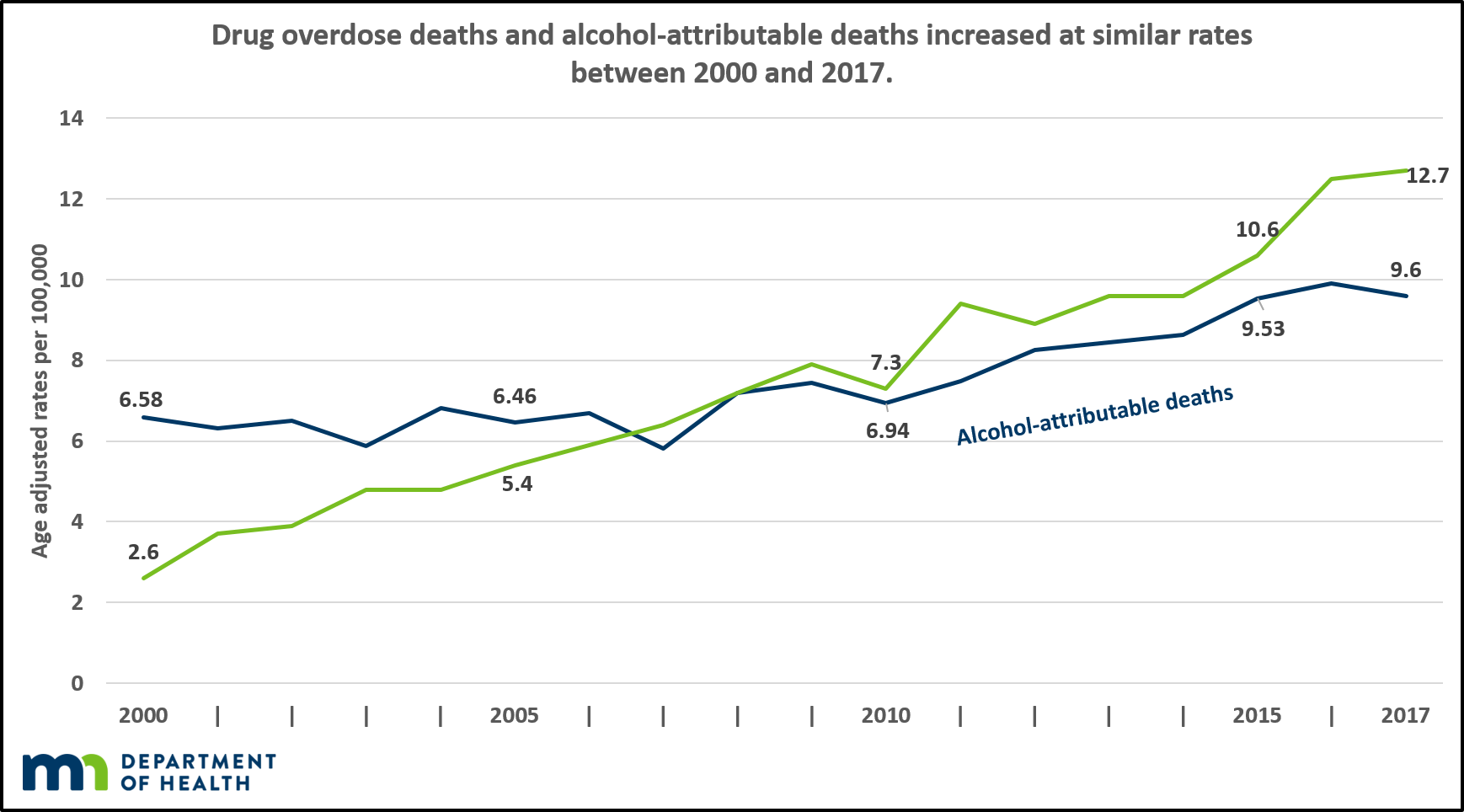
Between 2000 and 2017, 100% alcohol-attributable deaths almost doubled in Minnesota. The chart above shows the alcohol-attributable death rates and drug overdose deaths (age adjusted per 100,000) in Minnesota. While alcohol plays a role in a portion of drug overdose deaths, this chart shows the number of 100% alcohol-attributable deaths separate from these to show that 100% alcohol-attributable deaths increased at a similar rate as drug overdose deaths between 2000 and 2017.
Opioids
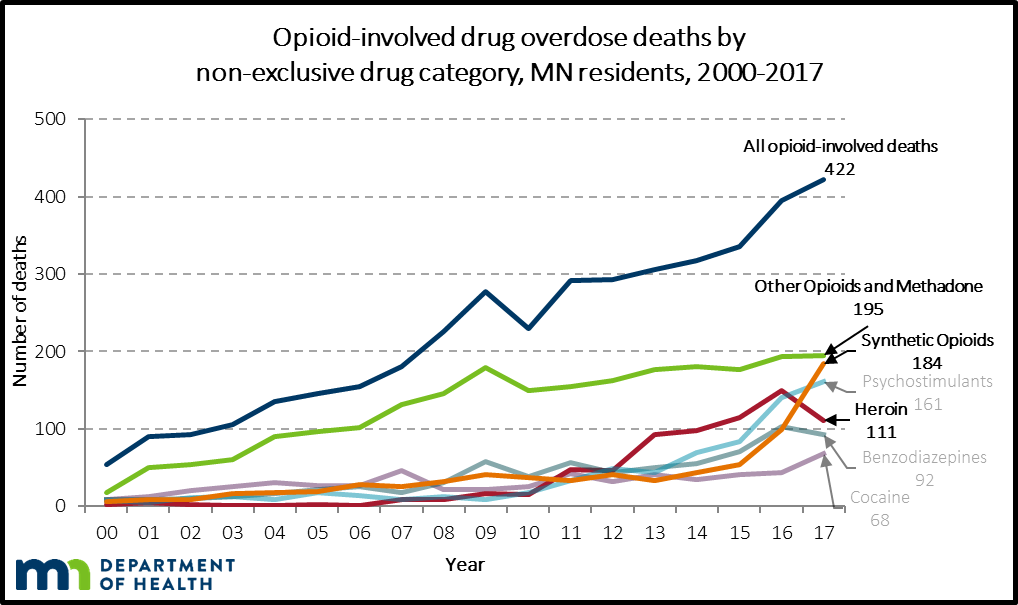
In 2017, opioid-involved deaths continued to increase for Minnesotans. From 2000 to 2017, opioid-involved deaths increased 681%. There was a 7% increase in opioid-involved deaths from 2016 to 2017:
- Other opioids and methadone (i.e. typically prescribed opioids, such as codeine, oxycodone, or hydrocodone) continue to cause the most opioid-involved deaths; there were 195 prescription opioid overdose deaths in 2017. This has remained stable over the past three years.
- From 2010-2016, heroin deaths increased rapidly, but they began to decline in 2017; there were 111 heroin-involved deaths in 2017 or a 26% decrease from 2016.
- Deaths from other synthetic opioids (e.g. fentanyl, fentanyl analogs, tramadol) have increased nearly 86% since 2016; there were 184 synthetic opioid- involved deaths in 2017.
Minnesota is unique in the fact that prescription opioids continue to account for the highest numbers of opioid-involved deaths. This is different than much of the rest of the country, which sees a majority of their opioid-involved deaths resulting from synthetic opioids.
Race-Rate Disparity
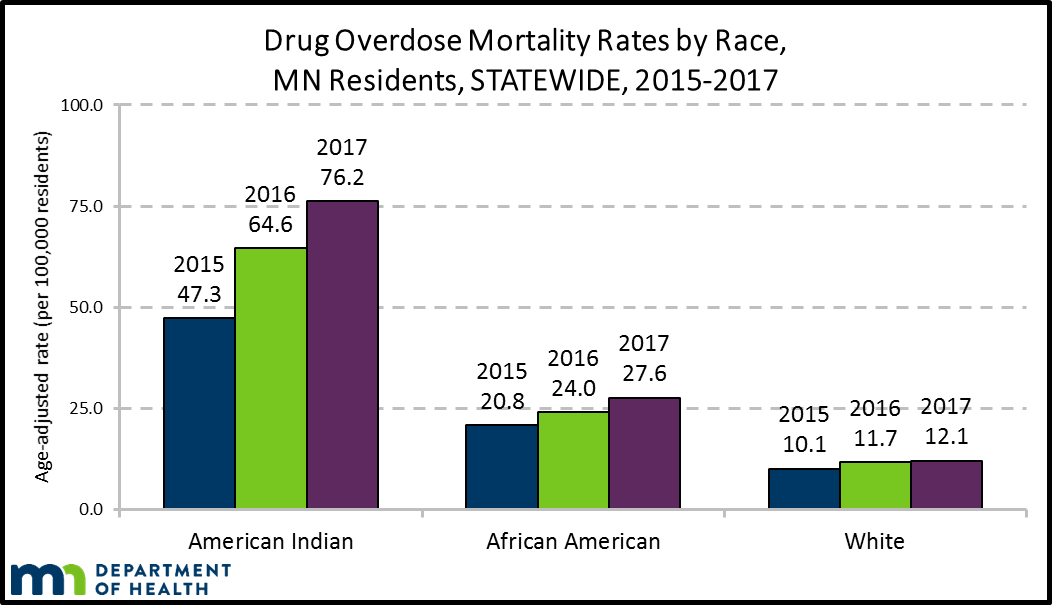
Historically, Minnesota has experienced the worst race-rate disparity in the nation for opioid-involved deaths among its American Indian population, and that remained true in 2017. The American Indian population represents 1.5% of the total population of Minnesota and 8% of all drug overdose deaths to Minnesota residents. Additionally, the race-rate disparity for opioid-involved deaths in African American Minnesotans was higher than many other states in 2017. The African American population represents 7% of the total population of Minnesota and 13% of all drug overdose deaths to Minnesota residents.
Final 2017 data shown in the chart above demonstrate that the disparity has continued and worsened. While the white drug overdose mortality rate increased from 11.7 to 12.1 per 100,000 white residents, the American Indian mortality rate increased from 64.6 per 100,000 residents to 76.2 per 100,000 residents, and the African American rate increased from 24.0 per 100,000 residents to 27.6 per 100,000 residents. Although national 2018 mortality data are not yet available, the disparity rate ratio is likely to remain among the highest in the United States.
Additional resources
- Alcohol-Related Deaths in Minnesota (PDF) data brief.
- Suicide in Minnesota, 1999-2017 (PDF)
- Drug Overdose Deaths among Minnesota Residents, 2000-2017 (PDF)
For more information
Contact Jon Roesler at Jon.Roesler@state.mn.us or
651-201-5487 for suicide-related data information.
Contact Kari Gloppen at kari.gloppen@state.mn.us for alcohol-related data information.
Contact Nate Wright at nate.wright@state.mn.us for opioid-related data information.